824
Views & Citations10
Likes & Shares
Obesity is a pandemic with many complications that increase the societal disease burden and cost of health care and decrease longevity and quality of life. Currently, 1 in 3 adults in the United States is obese. Physicians must therefore regularly confront obesity and its consequent diseases and develop strategies for effective treatment and management. This article summarizes current lifestyle modifications, pharmacological treatment and surgical options for the management of obesity and discusses the benefits, limitations and risks of each. As insights are gained into the pathophysiology of a gut-brain neurochemical feedback axis governing satiety and feeding behavior, targets for new pharmacotherapy are being developed. In particular, gut hormone analogs are an attractive anti-obesity therapy because they appear to lack the adverse effects historically associated with central nervous system-acting agents.
Keywords: Obesity, Metabolic syndrome, Pharmacological management, Co morbidity, Diabetes
INTRODUCTION
The societal and economic burden of obesity has reached pandemic proportions, with the World Health Organization (WHO) projecting a worldwide disease burden of 2.5 billion overweight adults and 700 million obese adults by 2015. In the United States, 1 in 3 adults is obese and the prevalence of obesity and obesity-related complications in childhood is increasing rapidly. In 2002, obesity accounted for >300,000 deaths and $117 billion in health care costs and loss of earning-related spending in the United States [1].
Obesity exacerbates or causes a number of debilitating, chronic medical conditions, including type 2 diabetes mellitus (T2DM), hypertension, dyslipidemia, coronary heart disease, stroke, osteoarthritis, obstructive sleep apnea, depression, gastro esophageal reflux disease, hepatic steatosis and gallbladder disease [2]. The prevalence of colon, endometrial, prostate and breast cancer has increased in parallel with the worldwide obesity pandemic. For all obesity-related diseases, risk increases with increasing body mass index (BMI) and decreases with successful weight reduction and maintenance of weight lost. Although there has never been greater need for effective obesity treatments, successful treatment remains a largely unrealized goal of global health care. Over the past few decades, academic medicine and the pharmaceutical industry have spent billions of dollars to identify and develop novel therapies to treat obesity. While there have been well-publicized drug failures, a number of candidate drugs are being researched. This article summarizes current treatment options and drugs in development for obesity [3-6].
LIFESTYLE INTERVENTIONS
Excessive calorie intake and a sedentary lifestyle promote weight gain, which leads to obesity. Lifestyle interventions such as food intake restriction, exercise and behavior modification form the cornerstone of obesity management. Weight gain or loss is directly related to the difference in energy intake and energy expenditure. Lifestyle interventions aim to increase the energy deficit and thereby promote weight loss. Such interventions continue to be the most successful nonsurgical treatment of obesity. Although a weight loss of up to 10% can be achieved using these approaches, poor adherence and recidivism (regain of lost weight) are significant problems. Following treatment, patients typically regain 30% to 35% of their lost weight in 1 year. Thus, all too frequently; the cornerstone of obesity management is missing [7,8].
DIETARY THERAPY
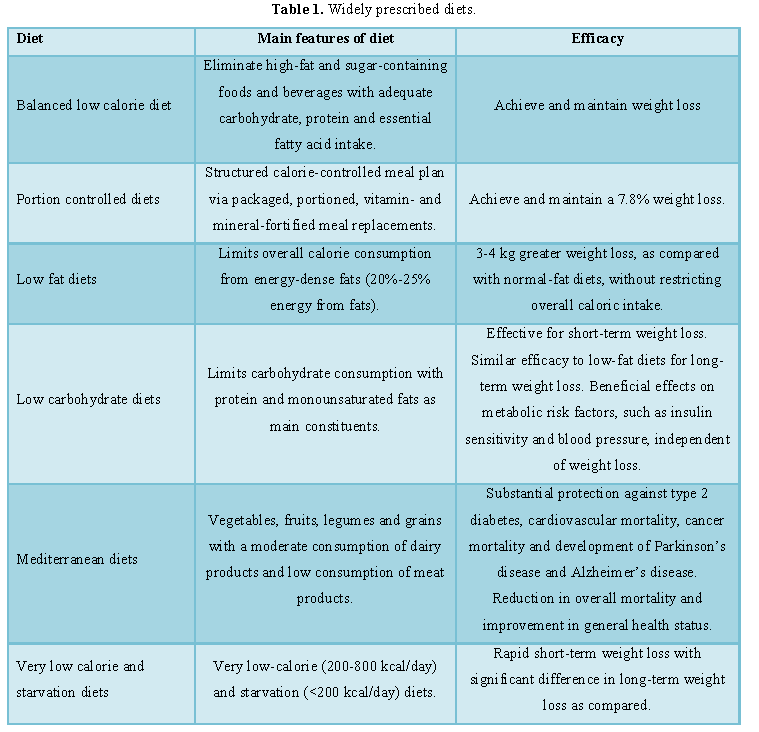
Dietary therapy for obesity seeks to restrict caloric intake. Data from animal research clearly links prolonged caloric restriction with increased lifespan [9]. There are a number of conventional hypo caloric diets that maintain energy intake >800 kcal/day but below daily energy expenditure requirements and unconventional diets, such as very low-calorie (
The more widely prescribed diets are summarized in Table 1.
EXERCISE THERAPY
A sedentary lifestyle promotes weight gain and early mortality in adults. Physical activity of any form can help protect against the development of obesity and has beneficial effects on metabolism and body composition [10,11]. As a single treatment for obesity, exercise therapy has been shown to be ineffective. Likewise, exercise therapy in combination with dietary therapy has not been shown to be superior to dietary therapy alone. The main established benefit of exercise in the management of obesity is the maintenance of weight loss after weight reduction. General advice to patients includes walking or cycling instead of driving and using stairs whenever possible to promote activity [12-15]. Health clubs and sporting activities may be helpful to facilitate exercise and motivate patients to undertake exercise regularly.
BEHAVIORAL THERAPY
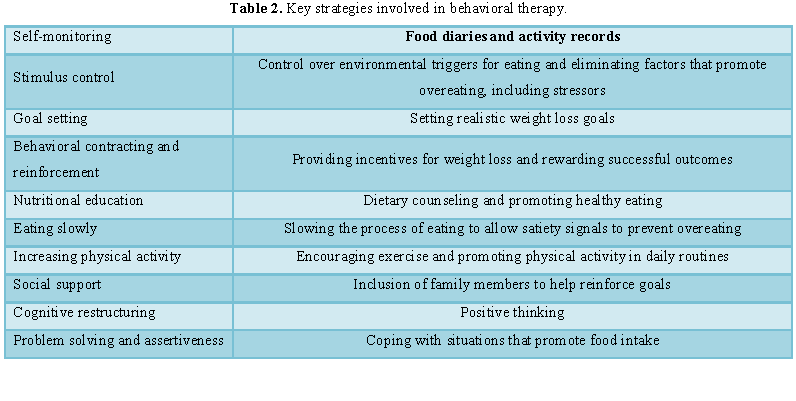
After completing a weight loss program, most obese patients regain lost weight. This may be due to recidivism, with resumption of previously accustomed poor eating patterns and sedentary lifestyle leading to weight gain. Behavioral therapy aims to change these lifelong habits that promoted weight gain into healthy eating and activity patterns that promote and maintain weight loss and seeks to provide the necessary support and motivation for obese patients to adhere to their weight loss program [16]. Behavioral therapy can improve initial weight loss and help maintain weight loss. The key strategies involved in behavioral therapy are summarized in Table 2. They can be delivered as part of individual or group therapy. In our experience, group therapy is more cost-effective [17].
PHARMACOLOGICAL TREATMENT
Over the past 25 years, >120 drugs have been investigated for the treatment of obesity. Only 1 drug in the United States, Orlistat, still has US Food and Drug Administration (FDA) approval for the long-term treatment of obesity. The other pharmacotherapy, including rimonabant and sibutramine, has been withdrawn from the market due to safety concerns. The efficacy of oral agents is modest, with placebo-subtracted weight loss of 2 who have failed to achieve weight loss goals through diet and exercise alone. We also advocate extending this recommendation to patients with a BMI of 27 to 29.9 kg/m2 and obesity-related co morbidity.
FDA-APPROVED PHARMACOTHERAPY FOR THE LONG-TERM TREATMENT OF OBESITY
Orlistat
Following the recent voluntary market withdrawal of sibutramine in the United States due to risks of serious cardiovascular events, Orlistat is now the only available long-term drug therapy for obesity in the United States and Europe. It is available as an over-the-counter medication in some countries, including the United States [21]. Orlistat is a pancreatic lipase inhibitor that is taken as a tablet with meals and results in reduced fat absorption by the digestive tract, leading to increased fecal fat excretion. The reduction of ingested fat absorption is dose dependent. At a maximal dose of 120 mg 3 times per day, up to 30% of ingested fat is excreted.
A number of clinical trials have demonstrated increased weight loss and reduced weight regain with Orlistat as compared with placebo. The mean weight loss difference between Orlistat and placebo at 12 months is 2.89 kg. Orlistat lowers hemoglobin A1C and serum lipids beyond what can be explained by weight loss alone [22,23].
There are no major safety concerns with Orlistat, but the drug does cause a number of gastrointestinal side effects. These include cramps, flatulence with borborygmi, fatty stools and fecal incontinence. Side effects are attenuated by avoidance of high-fat diets. Orlistat also reduces fat-soluble vitamin absorption due to its effects on fat absorption. Thus, supplementation of vitamins A, D and E may be prudent. Given its excellent safety profile, especially for patients with cardiovascular conditions, diabetes and dyslipidemia, we recommend Orlistat for drug therapy in obesity.
FDA-APPROVED PHARMACOTHERAPY FOR THE SHORT-TERM MANAGEMENT OF OBESITY
The short-term treatment of obesity is defined as ≤ 3 months [24]. These agents are unlikely to provide any long-term benefits because any weight lost during short-term therapy is likely to be regained after the treatment is stopped at 3 months.
Phentermine
Phentermine is an adrenergic reuptake inhibitor with both central nervous system (CNS) and peripheral effects as a de facto adrenergic agonist. It promotes weight loss by inhibiting food intake and increasing resting energy expenditure. In Europe, the license for Phentermine was withdrawn in 2001 following litigation. In the United States, it is a schedule IV controlled drug due to perceived potential for abuse, although evidence to substantiate that concern is lacking [25].
In a 36 week trial comparing continuous and intermittent Phentermine with placebo, both regimens resulted in greater weight loss compared with placebo (12.2 kg vs. 13 kg vs. 4.8 kg, respectively). Fenfluramine was used in combination with Phentermine (“fen-phen”) in the 1990s and this combination was effective in weight reduction. However, a high rate of cardiac valvular abnormalities was noted in patients taking this combination, which led to the withdrawal of Fenfluramine from the market. Phentermine monotherapy has not been linked to disproportionate incidence of cardiac valvular disease. As an adrenergic agonist, Phentermine use can cause or exacerbate tachycardia and hypertension and increase myocardial oxygen demand. Accordingly, it is advisable not to use this drug in patients with uncontrolled hypertension, known coronary heart disease or multiple coronary disease risk factors [26].
Diethylpropion
Diethylpropion is an orally administered anorectic agent which, like Phentermine, is an adrenergic agonist and schedule IV drug in the United States. It was withdrawn from European markets in 2001 for reasons similar to those cited in the removal of Phentermine [27].
FDA-APPROVED PHARMACOTHERAPY FOR RELATED CONDITIONS
While not indicated for obesity, several agents that promote weight loss are available for patients requiring treatment for T2DM, seizure disorders or depression.
T2DM medication
Type 2 diabetes mellitus is strongly associated with obesity. Moreover, in T2DM, glycemic control is worsened by weight gain and improved by weight loss [28]. Many effective anti-hyperglycemic agents, such as insulin, sulfonylureas and thiazolidinediones, have the undesirable effect of promoting weight gain in patients with diabetes, but a few agents do promote weight loss. These include metformin, the glucagon-like peptide-1 (GLP-1) agonists and pramlintide.
Metformin
Metformin is a biguanide that is currently advocated by the American Diabetes Association as initial monotherapy for T2DM. Metformin is a useful agent in the treatment of overweight patients with T2DM as it results in a mild but significant weight loss or prevention of weight gain [29]. A significant weight loss of 2.5% of body weight was also noted in patients with impaired glucose tolerance and the drug was associated with approximately 30% reduction in risk for developing T2DM in the Diabetes Prevention Program (DPP). However, clinical use in patients with impaired glucose tolerance for prevention of T2DM is still under further investigation and is not recommended at present. Lifestyle interventions were superior to metformin in preventing the onset of T2DM in the DPP.
GLP-1 receptor agonists: Exenatide and liraglutide
Glucagon-like peptide-1 is an incretin peptide that augments glucose-stimulated insulin secretion, reduces secretion of glucagon and delays gastric emptying. Exenatide and liraglutide are long-acting GLP-1 receptor agonists that are currently approved for the treatment of T2DM and have been associated with significant weight loss in T2DM clinical trials. Exenatide is associated with a 5.5 kg weight loss in 2 years [30]. Weight loss with liraglutide in 1 year was 2 to 2.5 kg, as opposed to a 1.1 kg weight gain with glimepiride. In a 26 week trial of liraglutide versus exenatide, weight loss was similar in both groups (3.24 vs. 2.87 kg). Dose-dependent nausea is a common side effect of these agents. Currently, exenatide is administered subcutaneously twice daily, while liraglutide is administered subcutaneously once daily. Exenatide long-acting release is a sustained-release formulation of exenatide, which is administered once weekly and is currently being studied in clinical trials, showing encouraging preliminary results.
Pramlintide
Pramlintide is a synthetic analog of amylin (i.e., islet amyloid polypeptide) that has recently been approved by the FDA for the treatment of type 1 diabetes mellitus (T1DM) and T2DM. Amylin is a peptide hormone co-secreted by β-cells along with insulin; its effects include slowing gastric emptying, promoting satiety and reducing postprandial glucagon secretion. It has been shown to improve glucose homeostasis in both T1DM and T2DM. In patients with T1DM, treatment with pramlintide for 1 year resulted in a 0.4 kg weight loss, as compared with a 0.8 kg weight gain with placebo. In patients with T2DM, treatment with pramlintide resulted in an additional 1.8 kg weight loss compared with placebo. Weight loss in patients with T2DM was more significant in patients with a BMI of >40 kg/m2 and in those concurrently treated with metformin.
ANTICONVULSANT MEDICATIONS
Topiramate
Topiramate is an anticonvulsant medication that is also approved for the treatment of migraine. A meta-analysis reported mean 6 month weight loss due to topiramate of 6.5% of initial body weight, with a placebo effect of 2%. Given its significant side effects and association with metabolic acidosis, further safety and efficacy trials are needed before recommending this agent for the primary indication of obesity.
Zonisamide
Zonisamide is an anticonvulsant with serotonergic and dopaminergic agonist activity. Weight loss with zonisamide was noted during clinical trials for its use in epilepsy. A trial of 60 subjects reported a 6.6% weight loss with zonisamide as compared with 1% with placebo at 16 weeks. After a 16-week extension of this trial with 37 subjects, weight loss was 9.6% for zonisamide and 1.6% for placebo. Further study of the safety and efficacy of this agent is needed before zonisamide can be recommended as a primary medical therapy for obesity.
ANTIDEPRESSANTS
Fluoxetine and sertraline
Fluoxetine and sertraline are selective serotonin reuptake inhibitors (SSRIs) used in the treatment of depression. A meta-analysis demonstrated that both agents may promote short-term weight loss (0.45 to 0.91 kg for sertraline and 0.4 to 14.5 kg for fluoxetine). In a longer-term trial of fluoxetine, there was a 50% weight regain between 6 months and 1 year. The very mild short-term weight loss and potential for weight regain long term make these agents ineffective primary anti-obesity treatments; however, they may be preferred as initial therapy for depression in patients with obesity.
Bupropion
Bupropion is an atypical antidepressant and smoking cessation aid. It acts primarily as a dopamine reuptake inhibitor, but is also an antagonist of norepinephrine and α3β4-nicotinic receptor antagonist. Bupropion produced a weight loss of up to 10.1% of initial body weight compared with 5% with placebo during a 24 week trial, with increased maintenance of lost weight at 48 weeks. Larger and longer-duration trials are needed before bupropion can be recommended as a primary obesity medication. Combinations of bupropion with other agents are currently undergoing clinical trials and are discussed later.
SURGICAL THERAPY
Bariatric surgery is indicated for obese patients with a BMI of >40 kg/m2, particularly when obesity-exacerbated health conditions are present. There are 3 basic types of surgical procedures (restrictive procedures, mal-absorptive procedures and mixed procedures), which vary in complexity and efficacy.
Restrictive procedures
Restrictive procedures restrict caloric intake by physically reducing the volume of the stomach lumen. Popular methods include laparoscopic adjustable gastric banding or laparoscopic vertical sleeve gastrectomy. Restrictive procedures are generally simpler with less operative risk and metabolic complications, but produce more gradual and less net weight loss as compared with mal-absorptive procedures.
Mal-absorptive procedures
Mal-absorptive procedures cause reduced intestinal absorption of nutrients by shortening functional small bowel length. One example of a mal-absorptive procedure is biliopancreatic diversion with duodenal switch. Compared with restrictive procedures, mal-absorptive procedures result in greater weight loss, but also have greater perioperative morbidity and greater potential for late postoperative metabolic complications.
Mixed procedures
Mixed procedures both restrict caloric intake and produce nutrient mal-absorption. Laparoscopic and open Roux-en-Y gastric bypass (RYGB) procedures are the most frequently performed mixed procedures and are comparable in both benefit and risk to mal-absorptive procedures.
BENEFITS AND RISKS OF BARIATRIC SURGERY
To date, bariatric surgical procedures have been shown to be the most effective treatment for obesity with regard to magnitude of sustainment of weight loss. As a result, bariatric procedures also produce improvement or remission in most obesity-associated diseases. The largest trial comparing surgical versus medical treatment of severe obesity is the Swedish Obese Subjects (SOS) trial. This study involved 4047 obese patients (BMI>34 kg/m2 for men and BMI>38 kg/m2 for women) and began in 1987. Of these patients, 2037 chose conventional treatment (non-standardized lifestyle ± medications) and 2010 underwent surgery, which included gastric banding, gastroplasty and gastric bypass. The study was nonrandomized but efforts were made to control for covariates. Weight decrease was significantly greater in the surgery group at 2 years (23% vs. 0.1%) and 10 years (16% vs. 0.16%) as compared with the control group. The incidence and control of T2DM, hypertension, hyperlipidemia, gastroesophageal reflux symptoms and obstructive sleep apnea improved in patients who underwent surgery. Quality of life was significantly improved and the number of medications and costs of medications per patient were significantly lower in patients who underwent surgery. There was a reduction in overall and cause-specific mortality in patients who underwent surgery.
Multiple observational studies support the concept that bariatric surgery is a highly effective, albeit costly, treatment for T2DM, with significant rates of remission of diabetes associated with all forms of bariatric surgery. In a meta-analysis of these studies, overall weight loss was 38.5 kg and complete remission of T2DM occurred in 78.1% of patients. Diabetes remission and weight loss rates were highest for mal-absorptive procedures and lowest for restrictive procedures. Diabetes resolution can occur rapidly after an RYGB procedure, prior to significant weight loss. It is thought that changes in gastrointestinal hormones following duodenal switch from RYGB surgery may account for this.
Based on aggregate data, perioperative mortality is <1% and adverse events occur in 20% of patients undergoing bariatric procedures. Major determinates of risk include patient comorbidities, experience and expertise of the surgeon and mean annual bariatric procedure volume of the center in which the procedure is being performed.
A National Institutes of Health (NIH) Consensus Development Panel in 1991 developed indications for bariatric surgery. The NIH considers bariatric surgery to be medically indicated (in conjunction with lifestyle management) for patients with a BMI of >40 kg/m2 or >35 kg/m2 when obesity-associated comorbidities are present and weight loss goals cannot be met with lifestyle management. The NIH panel advises that the risks, benefits and alternatives of surgery be clearly discussed so that an informed choice can be made by the patient and advocates that surgery be performed in a high-volume center by surgeons with extensive bariatric surgery experience. The NIH panel does not define high-volume centers or detail the amount of experience required by the surgeon. However, a recent study suggests that a mean annual bariatric procedure volume of
Although bariatric surgery is the most effective treatment for obesity, perioperative risk, financial cost and limited availability of surgical expertise and high-volume centers prevent it from becoming a universal solution to the obesity epidemic. At least 1 in 20 Americans is severely obese (BMI>40 kg/m2) and meets the NIH criteria for treatment of obesity with bariatric surgery. Only 0.6% of these eligible patients undergo bariatric surgery each year.
FUTURE PHARMACOTHERAPY OPTIONS
With the continuing increase in the prevalence of obesity and associated co morbidities, there is a great need for effective, safer and palatable treatment options. Research has identified a number of promising targets for drug therapy tailored to the pathophysiology of feeding, satiety and energy homeostasis. Given the problems with safety and adverse events from anti-obesity medications over the past few decades, new agents will need to demonstrate a satisfactory adverse event profile along with durable efficacy during clinical trials if they are to be approved as anti-obesity therapies. The FDA recently declined to approve a combination drug, Qnexa (Phentermine/topiramate), which demonstrated efficacy in producing weight loss, because there were concerns regarding long-term safety.
CNS-ACTING AGENTS IN LATE-STAGE CLINICAL TRIALS
Most medications in late-stage clinical trials are centrally acting drugs that interfere with the neurocircuitry involved in appetite and reward pathways. Adverse effects are to be expected, as neurotransmitter receptors are ubiquitous and spatially distributed in various CNS regions and peripheral tissues. The cannabinoid receptor antagonist rimonabant was a prototype of this class. Although selective for the CB1 receptor, this agent was associated with an untoward incidence of severe depression and anxiety, which led to its withdrawal from the drug market. Newer agents will undoubtedly be more selective ligands for receptors specifically involved in the neuroendocrine control of energy homeostasis, feeding and/or satiety.
GUT HORMONES FOR OBESITY TREATMENT
The gut-brain axis has received a lot of attention recently in the treatment of obesity because of its ability to regulate appetite and gut hormones. Gut hormones are major endocrine regulators of appetite and body weight. They hold promise of developing effective physiological anti-obesity therapies without the adverse event profiles of centrally acting agents.
Peptide YY
Peptide YY (PYY) is a hormone released from the L-cells of the gastrointestinal tract after a meal and in proportion to the number of calories ingested. PYY is the active form of PYY and promotes satiety, primarily via its central actions on the hypothalamus but also by delaying gastric emptying. Initial studies have utilized an injectable form of PYY, which has produced a reduction of food intake in humans. The most commonly known adverse effect is dose-related nausea. An intranasal formulation of PYY is currently in phase 2 clinical trials; however, results have been disappointing thus far, with high rates of nausea and limited efficacy.
Pancreatic polypeptide
Pancreatic polypeptide is secreted by PP cells within the islets of Langerhans in response to caloric intake. Infusion in lean, fasted humans reduced 24 h food intake by 25%. Pancreatic polypeptide shows a high affinity for the Y4 receptor, which is expressed in the appetite-controlling centers of the hypothalamus and has an effect on modulating NPY expression. Analogs to the Y4 receptor have been developed and are currently in phase 1 and 2 trials.
GLP-1/glucagon agonist
Glucagon is a peptide hormone secreted by the α-cells of pancreatic islets. On one hand, it raises blood glucose levels by stimulating glycogenolysis and gluconeogenesis; on the other hand, it reduces food intake. Its utility as obesity monotherapy has been compromised by its detrimental effects on glucose homeostasis and its short half-life. However, GLP-1 and glucagon receptors are similar in structure and in rodents, a long-acting co-agonist of GLP-1 and glucagon receptors produced weight loss greater than GLP-1 agonists alone without any adverse effects on glucose homeostasis. A co-agonist of glucagon and GLP-1 is currently in phase 1 clinical trials.
Ghrelin
Ghrelin is secreted by the stomach and gut hormones and is a potent stimulator of food intake. Ghrelin secretion increases prior to meals and falls in proportion to calories ingested. In obese subjects, an attenuated postprandial reduction in ghrelin has been reported. In theory, blocking this potent, naturally occurring, appetite-stimulating hormone could produce a useful therapeutic agent. Pharmaceutical companies are exploring the utility of ghrelin antagonists as well as inhibitors of the enzyme ghrelin O-acyl transferase, which is required to enable ghrelin to bind to its receptor, as potential anti-obesity treatments. An effective treatment is yet to emerge from ghrelin blockade.
CONCLUSION
The management of obesity presents a considerable challenge to physicians. The limited efficacy of lifestyle interventions has frustrated the medical community and patients alike. When combined with lifestyle interventions, pharmacological treatment is only slightly more effective than lifestyle intervention alone. The significant adverse event profile of some of these agents used in recent years has caused great concern and has led to the withdrawal of a number of anti-obesity therapies. At present, only 1 agent is approved for the long-term pharmacological treatment of obesity in the United States and Europe. Surgical options are more effective but carry a greater risk for adverse events as well as tremendous cost implications. They are only accessible to a limited number of patients. Drug therapies currently under development may allow us to utilize novel drug targets discovered over the recent years. A number of agents are currently in the drug development pipeline. It is hoped that future anti-obesity therapies based on selective ligands for neurotransmitter receptors involved in energy homeostasis and gut hormone-based treatments may offer a safer and more effective strategy to manage this growing problem.
1. World Health Organization (2006) Obesity and overweight fact sheet. Available online at http://www.who.int/mediacentre/factsheets/fs311/en/index.html
2. Flegal KM, Carroll MD, Ogden CL, Curtin LR (2010) Prevalence and trends in obesity among US adults, 1999-2008. JAMA 303: 235-241.
3. World Health Organization (2003) Global strategy on diet, physical activity and health. Available online at http://www.who.int/dietphysicalactivity/publications/facts/obesity/en/
4. (2002) Getting a handle on obesity. Lancet 359: 1955.
5. Bray GA (2004) Medical consequences of obesity. J Clin Endocrinol Metab 89: 2583-2589.
6. Field BC, Chaudhri OB, Bloom SR (2010) Bowels control brain: Gut hormones and obesity. Nat Rev Endocrinol 6: 444-453.
7. James WP (2008) The fundamental drivers of the obesity epidemic. Obes Rev 9: 6-13.
8. Wadden TA, Butryn ML, Wilson C (2007) Lifestyle modification for the management of obesity. Gastroenterology 132: 2226-2238.
9. Colman RJ, Anderson RM, Johnson SC, Kastman EK, Kosmatka KJ, et al. (2009) Caloric restriction delays disease onset and mortality in rhesus monkeys. Science 325: 201-204.
10. Freedman MR, King J, Kennedy E. (2001) Popular diets: A scientific review. Obes Res 9: 1S-40S.
11. Dansinger ML, Gleason JA, Griffith JL, Selker HP, Schaefer EJ (2005) Comparison of the atkins, ornish, weight watchers and zone diets for weight loss and heart disease risk reduction: A randomized trial. JAMA 293: 43-53.
12. Gardner CD, Kiazand A, Alhassan S, Kim S, Stafford RS, et al. (2007) Comparison of the atkins, zone, ornish and LEARN diets for change in weight and related risk factors among overweight premenopausal women: The A to Z weight loss study: A randomized trial. JAMA 297: 969-977.
13. Alhassan S, Kim S, Bersamin A, King AC, Gardner CD (2008) Dietary adherence and weight loss success among overweight women: Results from the A to Z weight loss study. Int J Obes (Lond) 32: 985-991.
14. Sacks FM, Bray GA, Carey VJ, Smith SR, Ryan DH, et al. (2009) Comparison of weight-loss diets with different compositions of fat, protein and carbohydrates. N Engl J Med 360: 859-873.
15. Williamson DF, Madans J, Anda RF, Kleinman JC, Kahn HS, et al. (1993) Recreational physical activity and ten year weight change in a US national cohort. Int J Obes Relat Metab Disord 17: 279-286.
16. Katzmarzyk PT, Church TS, Craig CL, Bouchard C (2009) Sitting time and mortality from all causes, cardiovascular disease and cancer. Med Sci Sports Exerc 41: 998-1005.
17. Slentz CA, Duscha BD, Johnson JL, Ketchum K, Aiken LB, et al. (2004) Effects of the amount of exercise on body weight, body composition and measures of central obesity: STRRIDE - A randomized controlled study. Arch Intern Med 164: 31-39.
18. Miller WC, Koceja DM, Hamilton EJ (1997) A meta-analysis of the past 25 years of weight loss research using diet, exercise or diet plus exercise intervention. Int J Obes Relat Metab Disord 21: 941-947.
19. Ross R, Dagnone D, Jones PJ, Smith H, Paddags A, et al. (2000) Reduction in obesity and related comorbid conditions after diet-induced weight loss or exercise-induced weight loss in men. A randomized, controlled trial. Ann Intern Med 133: 92-103.
20. Jakicic JM, Marcus BH, Lang W, Janney C (2008) Effect of exercise on 24 month weight loss maintenance in overweight women. Arch Intern Med 168: 1550-1560.
21. Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, et al. (2009) American College of Sports Medicine. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc 41: 459-471.
22. National Institutes of Health: National Heart, Lung and Blood Institute and North American Association for the Study of Obesity (2000) The practical guide: Identification, evaluation and treatment of overweight and obesity in adults. NIH publication.
23. Centre for Disease Control and Prevention (2004) Prevalence of overweight and obesity among adults with diagnosed diabetes-United States, 1988-1994 and 1999-2002. MMWR Morb Mortal Wkly Rep 53: 1066-1068.
24. Svetkey LP, Stevens VJ, Brantley PJ, Appel LJ, Hollis JF, et al. (2008) Comparison of strategies for sustaining weight loss: The weight loss maintenance randomized controlled trial. JAMA 299: 1139-1148.
25. Rucker D, Padwal R, Li SK, Curioni C, Lau DC (2007) Long term pharmacotherapy for obesity and overweight: Updated meta-analysis. BMJ 335: 1194-1199.
26. Padwal R, Li SK, Lau DC (2004) Long-term pharmacotherapy for obesity and overweight. Cochrane Database Syst Rev 2004: CD004094.
27. Kaya A, Aydin N, Topsever P, Filiz M, Oztürk A, et al. (2004) Efficacy of sibutramine, orlistat and combination therapy on short-term weight management in obese patients. Biomed Pharmacother 58: 582-587.
28. Snow V, Barry P, Fitterman N, Qaseem A, Weiss K (2005) Pharmacologic and surgical management of obesity in primary care: A clinical practice guideline from the American College of Physicians. Ann Intern Med 142: 525-531.
29. Zhi J, Melia AT, Guerciolini R, Chung J, Kinberg J, et al. (1994) Retrospective population-based analysis of the dose-response (fecal fat excretion) relationship of orlistat in normal and obese volunteers. Clin Pharmacol Ther 56: 82-85.
30. Li Z, Maglione M, Tu W, Mojica W, Arterburn D, et al. (2005) Meta-analysis: Pharmacologic treatment of obesity. Ann Intern Med 142: 532-546.
-
 Table 1
Table 1 -
Table 2
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Surgery and Invasive Procedures (ISSN:2640-0820)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- Journal of Cardiology and Diagnostics Research (ISSN:2639-4634)
- Journal of Alcoholism Clinical Research
- Journal of Spine Diseases


